


PROFESSOR GERALD B. FOGARTY
Sydney Radiation Oncologist with an interest in Skin Cancer & Benign Skin Conditions
The purpose of this website is to help patients and their families understand the rationale, process and side effects of radiation treatment of skin conditions, especially through the experience and published work of Prof Fogarty.
Prof Fogarty works at The Icon Cancer Centres at Wahroonga, and Gosford which includes a peripheral site at Wyong.
The Icon Cancer Centre - Wahroonga
Level 2, Clark Tower, Sydney Adventist Hospital
185 Fox Valley Road, Wahroonga NSW 2076
Phone. (02) 9480 4200
Fax. (02) 9487 9303
Email. gerald.fogarty@icon.team
Admin Email: admin.wahroonga@icon.team
Parking: There is parking at the Hospital. Carpark One level 2 is the closest parking. Buses from Turramurra, Thornleigh and Hornsby station serve the Hospital.
The Icon Cancer Centre - Gosford
41 William Street
Gosford NSW 2250.
Phone. (02) 4349 8000
Fax. (02) 4324 6121
Email. gerald.fogarty@icon.team
Admin Email: admin.gosford@icon.team
The Icon Cancer Centre - Wyong
Tuggerah Lakes Private Hospital
Cnr Pacific Highway & Craigie Avenue
Kanwal NSW 2259
Appointments are made through the ICON Gosford contact details.
Prof Fogarty is a member of the SAN Skin Cancer, Sarcoma and Melanoma multidisciplinary team (MDT) and the Gosford Hospital Skin MDT.
Why Choose Radiotherapy?
Radiotherapy can treat a mixed population of normal cells and tumour cells, kill the tumour cells but leave the normal cells unharmed.
Radiotherapy results in tissue conservation - see lip cancer example below.
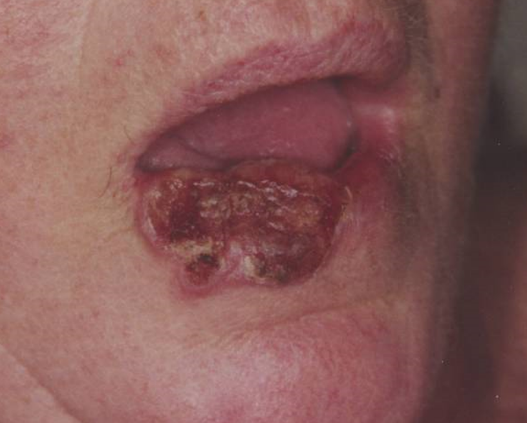
Large neglected cSCC of Lip

Six months after Radiotherapy alone
No surgery was used
The need for Fractionation

Table comparing Radiotherapy and Surgery
Radiation needs to be given in small amounts over time in order to deliver an excellent cosmetic and functional outcome. This is called fractionation. Fractionation describes how the total radiation dose is given in smaller partial doses, often daily. Fractionation allows normal tissue to survive radiation while the tumour cells in the same volume die. This is because normal cells have good radiation repair mechanisms while tumour cells do not. After a small dose of radiation, the normal cells can repair while the tumour cells cannot. The tumour cells die. Most repair happens in the first 6 hours following radiation treatment.
We are actively researching new biological ways to decrease the number of fractions and therefore decrease the number of visits to the radiotherapy department, to make the treatment experience easier on patients. One of them in mainstream practice now is the Adaptive split course radiotherapy (ASCRT) (Fogarty GB, Br J Dermatol. 2018)”
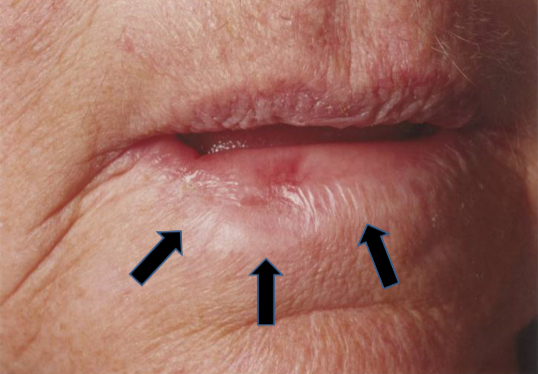
This lip example shows what happens when there is not enough fractionation. These figures show a patient who had an upper right lip cancer treated with radiotherapy. These photos have been taken some years after treatment. One can see that there are several problems even though the cancer is cured. The area has decreased coloration. This is called hypopigmentation. There are also blood vessels visible, this these are called telangiectasia. There is also a decrease in the amount of tissue and the tissue is hardened. This is called cicatrization.
These side effects are caused by increased fibrosis as the fraction size has been too big, meaning that the repair capacity of the normal cells has been exceeded and normal cells have died and have been replaced by fibrous tissue within the radiation field. These side effects are avoided with adequate fractionation. The second figure shows the same person with who is now smiling. One can see that this these late effects from the radiotherapy have caused a functional deficit in the way this person smiles.
Comparison of Radiotherapy & Surgery
How is Radiotherapy similar to Surgery?
Definitive radiotherapy and surgery are both local treatments. They have similar cancer control ability, although further prospective comparative study is required.
How is Radiotherapy different from Surgery?
Radiotherapy is different from surgery in a number of ways. Surgery always removes tissue. Radiotherapy always conserves tissue. Tissue conservation leads to a better functional and cosmetic effect, resulting in better survivorship. Radiotherapy is therefore particularly useful when tissue conservation is important eg. face, nose, ears, eyelids, genitals, fingers and toes. Radiotherapy has no pain on delivery so there is no need for anaesthetic. There is no tissue removal, and so no need for grafting, and so no need for an in-patient stay, for example, with the leg up for the surgery to heal. As there is no cutting, anticoagulation does not need to be stopped prior to treatment. Radiotherapy is delivered over time and may require many visits. As no tissue is removed there is no histopathology report. There are short term side effects, usually, at the end of treatment, that may require temporary nursing care until healed.

Table comparing Radiotherapy and Surgery
Recent improvements in RT have come from better physics and understanding of radiobiology
Improvements that Prof Fogarty is working on include new technologies such as “flash” treatments, the use of heat, and the investigation of the metallic content of the tumours. These projects are under investigation with international consortia and will be presented at conferences and published as soon as the results are mature and analysed.
The Radiation Treatment Journey
Prof Fogarty heads up a radiation multidisciplinary team. Radiation nurses with a specific interest in skin cancer, radiation therapists also with a specific interest in skin cancer and specific training for that, and radiation physicists who will help to design the radiation fields and the appropriate filtration needed. All combine their skills to maximize your experience from all angles. All have a specialised role, all are important and you will meet them on your journey.
Your radiation journey begins with having a consultation with Prof Fogarty. A referral from a doctor is needed. GPs can refer. A new patient appointment can be made by ringing the relevant department listed above and asking for an appointment with Professor Fogarty.
Radiation for Cancers of the Skin
Cancers that can be treated with radiation include basal cell carcinoma (BCC), cutaneous squamous cell carcinoma (cSCC), Melanoma, Merkel Cell Carcinoma (MCC), Lymphoma and a range of rarer tumours such as malignant fibrous histiocytoma (MFH) etc.
BCC and cSCC are sometimes called keratinocytic cancers as they both come from the same cell, the keratinocyte.
All skin cancers that are not melanoma can be described by the term non-melanoma skin cancers or NMSC, but this term is being phased out.Invasive disease is capable of spreading to other organs. The mode of spread can be by local invasion into other organs. This is the usual mode of spread for BCC. It can be by perineural invasion. It can be by lymphovascular space invasion, spreading to nearby lymph nodes, and then into the rest of the body.
Some cancers have a non-invasive phase, also called an in-situ phase. cSCC has various names for its in-situ stage, which include in-situ cSCC, Bowens Disease and intraepithelial carcinoma, they are really all the same thing. Melanoma also has various names for its in-situ stage which include in-situ melanoma, Hutchinson Melanotic Freckle (HMF) and Lentigo Maligna, again really all the same thing. Adenocarcinoma of skin has as its in-situ phase extramammary Paget’s disease (EMPD). The non-invasive phase is considered dangerous as it can progress to invasive disease.
Radiation for Benign Conditions of the Skin
These are not cancer but are troublesome because they have a population of cells that divide regularly when they should not, causing symptoms. Radiotherapy is effective because it slows the pace of cell division.
Benign conditions include Rosacea, Keloid, Psoriasis, Extramammary Pagets Disease (EMPD), hidradenitis suppurativa (HS), Disseminated Superficial Actinic Porokeratosis (DSAP) can be treated with radiotherapy.
What is the Intention of Radiation Treatment?
Definitive treatment is when radiation is the main treatment. It is usually used alone to cure.
Adjuvant radiation is when radiation is used as a guarantee following another therapy that has unexpectedly not worked so well eg RT after surgery when the surgery has not cleared all the cancer.
Palliative treatment is when RT is used to reduce symptoms such as pain, bleeding, the need for dressings, and smell. It stops the cancer having such a great impact on function and cosmesis.
